3rd Entry - Summary of all Cases
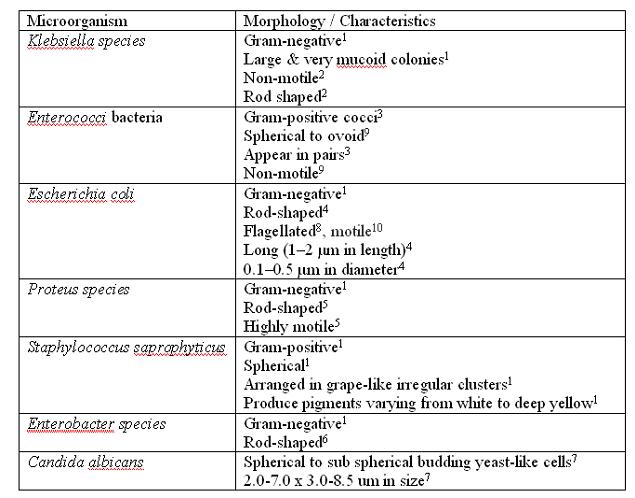
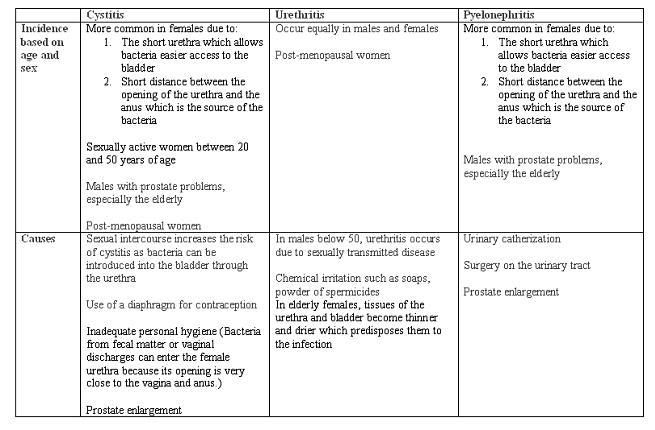
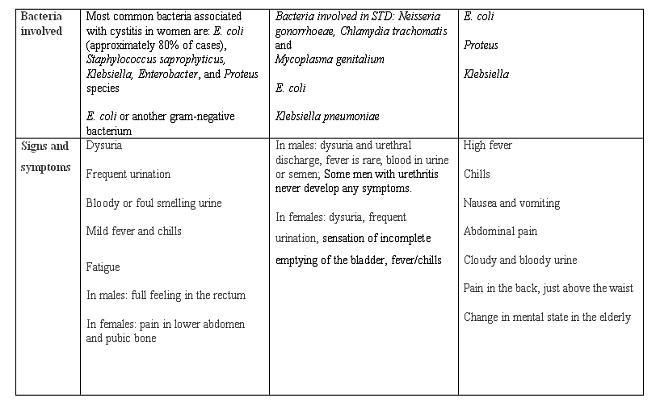
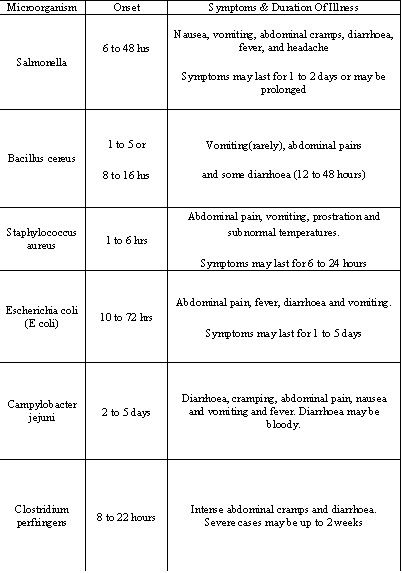
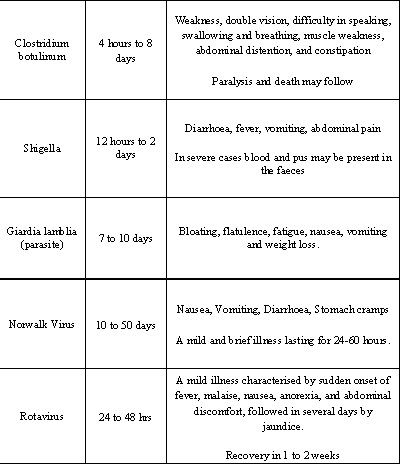
All the necessary information is collated by all members and organised into tables. This can be seen below.

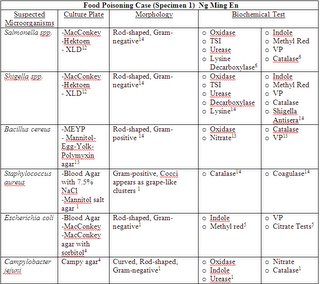

Abbreviations:
IMVic: indole-methyl red-Voges-Proskeur-Citrate
ONPG: O-nitrophenyl-β-D-galactopyranoside
OF: oxidation-fermentation
TSI: triple sugar iron
VP: Voges-Proskeur
MR: Methyl Red
References:
(1) http://findarticles.com/>
(2) http://medinfo.ufl.edu>
(3) http://tucom.bigbri.net/>
(4) http://en.wikipedia.org/>
(5) http://www.umm.edu/>
(6) http://textbookofbacteriology.net>
(7) Gabriel Virella. Microbiology and infectious diseases. Third edition
(8) http://w3.ouhsc.edu/>
(9)http://www.microbelibrary.org>
(10) http://members.tripod.com
(11) http://www.mc.maricopa.edu/>
(12) http://www.who.int/>
(13) http://www.rci.rutgers.edu/>
(14) G.Brooks, J.Butel and S.Morse. (2004). Jawetz, Melnick & Adelberg’s Medical Microbiology
(15) Henry D. Isenberg. Essential procedures for clinical microbiology



Abbreviations:
IMVic: indole-methyl red-Voges-Proskeur-Citrate
ONPG: O-nitrophenyl-β-D-galactopyranoside
OF: oxidation-fermentation
TSI: triple sugar iron
VP: Voges-Proskeur
MR: Methyl Red
References:
(1) http://findarticles.com/>
(2) http://medinfo.ufl.edu>
(3) http://tucom.bigbri.net/>
(4) http://en.wikipedia.org/>
(5) http://www.umm.edu/>
(6) http://textbookofbacteriology.net>
(7) Gabriel Virella. Microbiology and infectious diseases. Third edition
(8) http://w3.ouhsc.edu/>
(9)http://www.microbelibrary.org>
(10) http://members.tripod.com
(11) http://www.mc.maricopa.edu/>
(12) http://www.who.int/>
(13) http://www.rci.rutgers.edu/>
(14) G.Brooks, J.Butel and S.Morse. (2004). Jawetz, Melnick & Adelberg’s Medical Microbiology
(15) Henry D. Isenberg. Essential procedures for clinical microbiology
posted by SyafiqaH @ 5:01 AM
2 comments
![]()







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}