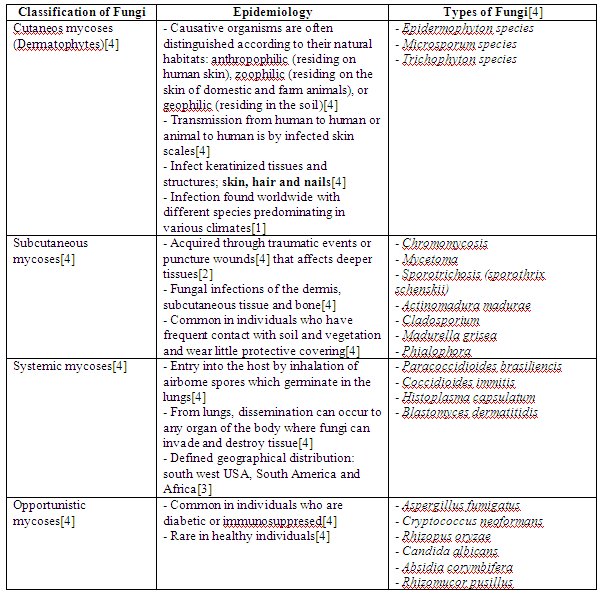
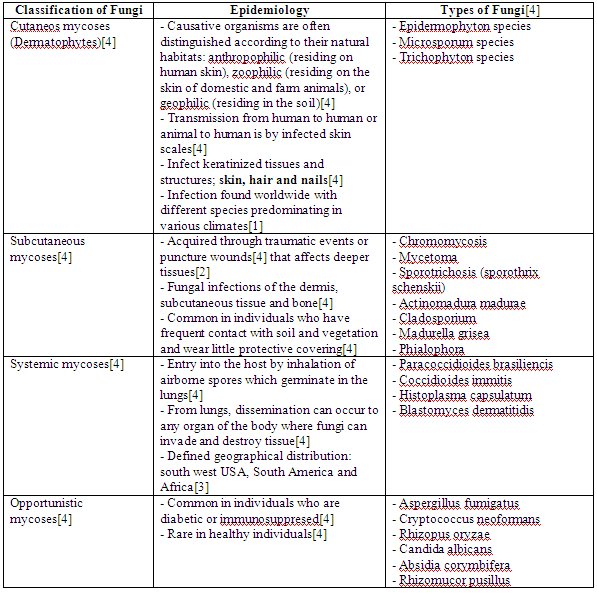
FungusThere are many different classifications of fungus and parasites. The classification of fungi is summarized in the table below:

From the table above, the most possible cause of fungal infection for soldiers is
cutaneous mycoses (dermatophytes). This is so as it is mainly
caused by lack of hygiene practices, which may be common for soldiers.
In contrast, subcutaneous mycoses is more common for people who does plantation as it usually present in individuals who have frequent contact with soil and vegetation[4]. It is also unlikely that the soldiers can be infected by systemic mycoses as the defined geographical distribution excludes South East Asia countries. Opportunistic mycoses will also probably not infect soldiers as it is only common in individuals who are diabetic or immunosuppresed[4].
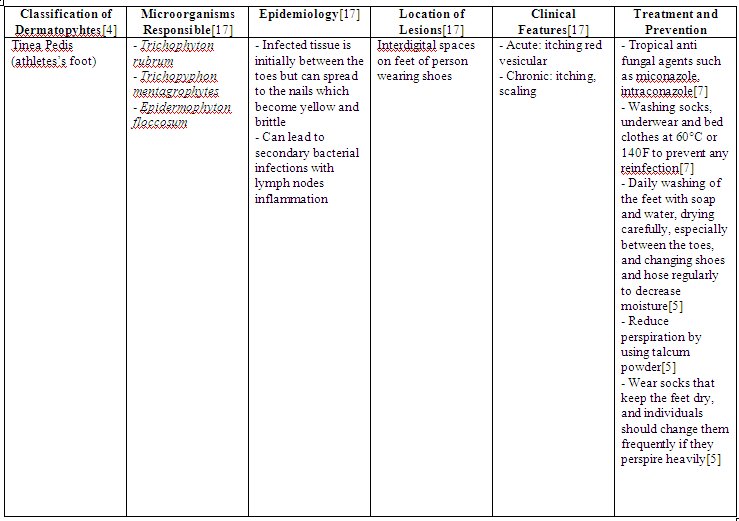
Now that dermatophytes is identified as the most possible cause of fungal infections for soldiers, we should then evaluate classification of this class of fungal infection. This can be summarized in the tables shown below:



From the table above, the main genres include
Trichophyton, Microsporum and Epidermophyton.Reasons how this fungus can infect soldiers:
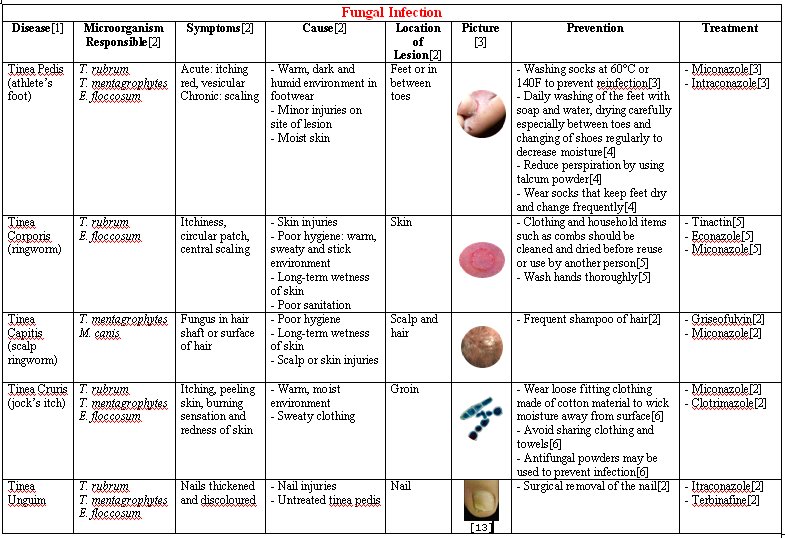
Tinea Pedis (athlete’s foot):Soldiers will usually put on shoes for long hours each day. The fungus will most often attack the feet because shoes create a
warm, dark, and humid environment, which encourages fungus growth [5]. If the feet are not washed adequately with soap and water, the fungus may
continue to spread to the soles of the feet and to the toenails[5].
Tinea corporis (ringworm):This fungus thrives in warm, moist areas.
Poor hygiene, long-term wetness of the skin (such as from sweating) and
minor skin and nail injuries usually raise the risk for a fungal infection. Tinea corporis is contagious when there is a direct contact with someone who is infected, or if in touch with contaminated items such as combs, clothing, shower floors and walls, or pool surfaces [11]. Soldiers usually experience poor sanitation and are usually in a warm, sweaty and sticky environment. Since it is
contagious thus it will spread among the soldiers easily and by sharing contaminated items, it would increase the risk of the above fungal infection.
Tinea Cruris (“jock itch”):Soldiers perspire often, creating a warm and moist environment for the fungus to grow. Causes of Tinea Cruris includes
wearing sweaty or wet clothing[6]. Soldiers may also share clothes and towels. This is a possible cause of getting jock itch[6].
Tinea capitis (scalp ringworm):An individual may have an increased risk for tinea infection if they have
poor hygiene, prolonged wetness of the skin and minor skin or scalp injuries[11]. Prolonged wetness of the skin on the scalp may be due to the
long period of time in wearing of the barret or helmet. Like Tinea corporis (ringworm), scalp ringworm are also contagious and a soldier may get infected if he
come into direct contact with another soldier who has the condition, or by touching contaminated items such as combs, barret or clothing[11].
Tinea unguium (onychomycosis):
Onychomycosis is due to a
fungal infection of the nail. Occasionally, fungal infection of the feet can lead to the nails becoming infected[20]. Tinea unguium often results from untreated tinea pedis(feet)[21]. When the soldiers encounter tinea pedis, it is usually left untreated for quite some time and this could result in the rise of tinea ungium.
ParasiteThere are 3 main class of parasites that can cause infection to soldiers. This includes protozoa, helminths and scabies.
ProtozoaProtozoa can be classified based on the site of infection. This can be summarized in the table below:

* Amoebas: move by extending cytoplasmic projections
Flagellates: move by rotating whip-like flagella
Sporozoa: generally have non-motile adult forms
From the table above, it seems that
Trypanosome species and
Leishmania species can be ruled out as they are not commonly found in Asia.
Plasmodium species can also been ruled out because based on our further research, Brunei has declared to be a malarial-free country, and thus it is least likely to have
plasmodium species.
Trichomonas vaginalis has also been ruled out as it is usually sexually transmitted. As for
Cryptosporidium parvum, it has been rule out as well because it is more common when in direct contact with farm animals. As the cat (undercooked meat) is the definitive host for
Toxoplasma gondii, it is ruled as well.
Thus the species that are possible for this situation would be
Entamoeba histolytica,
Giardia lamblia and
Cyclospora cayetanensis.
Reasons how these protozoa can infect soldiers:
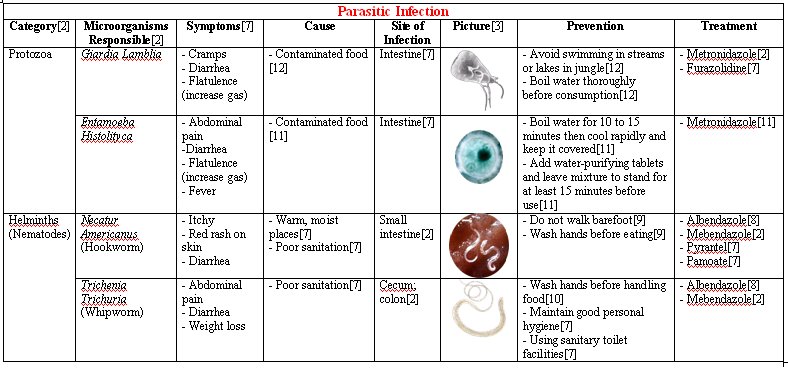
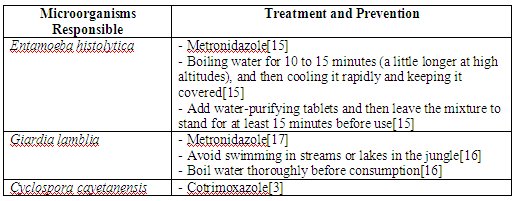
Entamoeba histolytica:
Entamoeba histolytica causes amoebic dysentery and is endemic in many
tropical countries, but it is attributable more to
unsanitary conditions than to heat[15].
Due to unsanitary conditions in the jungle, amoebic dysentery is most commonly spread by
water or contaminated, uncooked food or from carriers. Flies may carry the cysts to spread the amoeba from the feces of infected persons to food[15].
Giardia lamblia (Giardia intestinalis):
Giardia lamblia is found in
soil, food, water, or surfaces that have been contaminated with the feces from infected humans or animals. It is common during travel to less developed countries in Southeast Asia[16].
With unsanitary conditions in the jungle, food might not be properly cooked and this could cause the transmission of Giardia lamblia. In addition, outbreaks among military personnel in the wilderness could also be due to an
infection with various animal giardia harboured by animals such as rodents[17].
Cyclospora cayetanensis:
Cyclospora cayetanensis is common in the tropics as
warm and moist environment is essential before the oocyst sporulate into their infective form[13].
Transmission occurs in military personnel through the
consumption of contaminated food and water[14].
The treatment and prevention of these microorganisms are summarised in the table below:
 Helminths
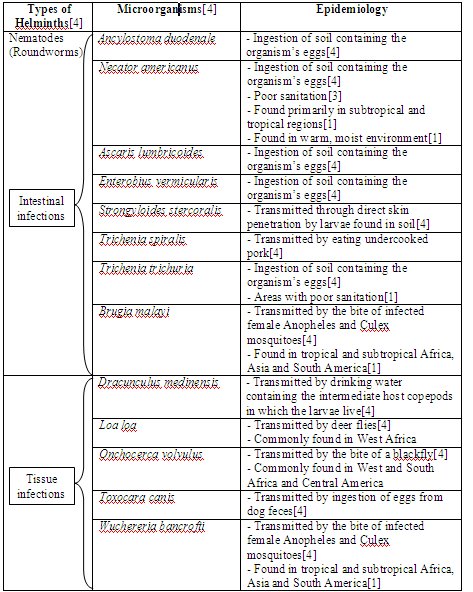
Helminths Helminths are worms, some of which are parasitic to humans[4]. The different types of helminths and microorganisms responsible are shown in the table below:

The epidemiology of the aboved microorganisms is summarised in the tables below. This is to exclude the microorganisms that is less possible to cause infection to soldiers.


From the table above, we have excluded most of the microorganisms and left with
Necatur americanus (hookworm) and Trichenia trichuria (whipworm) as they are the
most common microorganisms that could infect the soldiers.
Cestodes family also known as tapeworms are eliminated as they are due to undercooked meat (i.e: fish, pig, beef and etc.) and in this case we find that they seldom occur to the soldiers as they are often serve with food rations. Thus in this case, it is least likely to occur.
As for the Trematodes genre or also known as Flukes, they are also ruled out as based on their areas commonly found, none of them are commonly found in South East Asia. Thus, it is least likely to appear in Brunei jungle.
Nematodes genre or also known as the roundworms, only two species are specifically chosen. The other microorganisms are ruled out based on how they are transmitted or where they are commonly found.
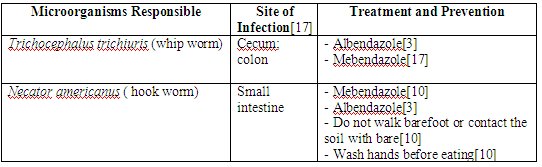
The site of infection, treatment and prevention of these helminths (hookworm and whipworm) are summarised in the table below:
 Reasons how these helminths can infect soldiers: Whip worm (Trichocephalus trichiuris):
Reasons how these helminths can infect soldiers: Whip worm (Trichocephalus trichiuris):Whipworm infection is very common in
tropical areas where there is
poor sanitation[12]. Warm climates provide the conditions for whipworm eggs to incubate in the soil[12].
Military personnel involved in jungle training most probably did not live in sanitary conditions and personnel could have acquired the parasite when they
consume food that has been contaminated with eggs
Hookworm (Necator americanus):
Hookworm is most common in
warm, moist places where sanitation is poor, such as the jungle. Two species of hookworm cause infection in people:
Ancylostoma duodenale, which is present in India, China, Japan, and the Mediterranean area; and
Necator americanus, which is present in the tropical areas of Africa, Asia, and the Americas[12]. Hence, the most likely species of hookworm infection commonly encountered by military personnel are of the
Necator americanus species, as jungle training took place in Brunei.
Larvae emerge to live in the soil. When fully developed, the larvae can penetrate the skin. A person can become infected by
walking barefoot or sitting in contaminated soil[12]. Infection may also occur when
foods contaminated with hookworm cysts are eaten[8].
Hookworm eggs are passed in stool and infection results when a person comes in contact with the eggs from the contaminated soil, stool or water[9].
Military personnel are often protected against hookworms as they are fully clothed without any exposure of their skin. However, if their skin is exposed to soil during physical training, it would predispose them to hookworm infections as the larvae can penetrate through their skin.
ScabiesScabies (Sarcoptes scabiei):Scabies is a skin condition caused by a burrowing mite known as
Sarcoptes scabiei[7]. It is a very contagious parasite which can spread easily through an infected individual through to other people. The infestation of this parasite is common, found worldwide, and affects people of all races and social classes[18]. It spreads more easily in crowded situations.
As army soldiers
share the same tents, and are involved in many different physical activities, physical contact with one another would be a norm thus promoting the transmission of scabies throughout the entire population.
Treatment and Prevention:- Avoid sharing common objects like clothing and bedding etc[7].
- Application of permethrin or oral dose of Invermectin for treatment[7].
References[1] Tom Elliot, Mark Hastings and Ulrich Desselberger. Lecture notes on medical microbiology. 3rd edition. 1997. Blackwell science
[2] Medical microbiology lecture notes. Teamsek Applied Science School
[3] Stephen Gillespie and Kathleen Bamford. Medical microbiology and infection at a glance. 2000. Blackwell science
[4] Richard A. Harvey, Pamela C. Champe and Bruce D. Fisher. Microbiology. 2nd edition. 2006. Lippincott Williams and wilkins
[5] http://www.apma.org>
[6] http://dermatology.about.com>
[7] http://wikipedia.org>
[8] http://www.jhhs.org>
[9] http://www.personalmd.com>
[10] http://www.dpd.cdc.gov>
[11] http://www.nlm.nih.gov>
[12] http://www.merck.com>
[13] http://www.doh.state.fl.us>
[14] http://www.parasite-cleanse.com>
[15] http://www.mayaparadise.com/>
[16] http://www.answers.com>
[17] Brooks, G. F., Butel, S. F., and Morse, S. A. (2004). Jawetz, Melnick & Adelberg’s Medical Microbiology (23rd ed.). Singapore: McGraw-Hill.
[18] http://www.cdc.gov>
[19] http://www.umm.edu>
[20] http://www.ecureme.com>
[21] http://dermnetnz.org>
(The contents of this entry are contributed by all members. Tables are organised by Yasmin)

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}